If a dentist told you that you don’t have enough bone for implants, you probably walked out feeling like the door closed.
It usually didn’t.
I see this pattern in my office regularly. A patient comes in for a second opinion. They had a consult somewhere else, were told their bone is too thin or too short, and were handed a treatment plan for dentures or a partial. Sometimes that’s accurate. Often it isn’t. The dentist they saw may not place implants in complex cases, or didn’t have the 3D imaging to plan around the limitation, or simply hadn’t trained in the techniques that work when bone is the problem.
I’m Christopher J. Manduzzi, DDS, a Fellow of the International Congress of Oral Implantologists. I’ve been planning and placing implants out of my office in historic downtown Utica for years. This post walks through what “not enough bone” actually means, the real options available in 2026, and what to ask before you accept that implants are off the table.
Why Bone Disappears In the First Place
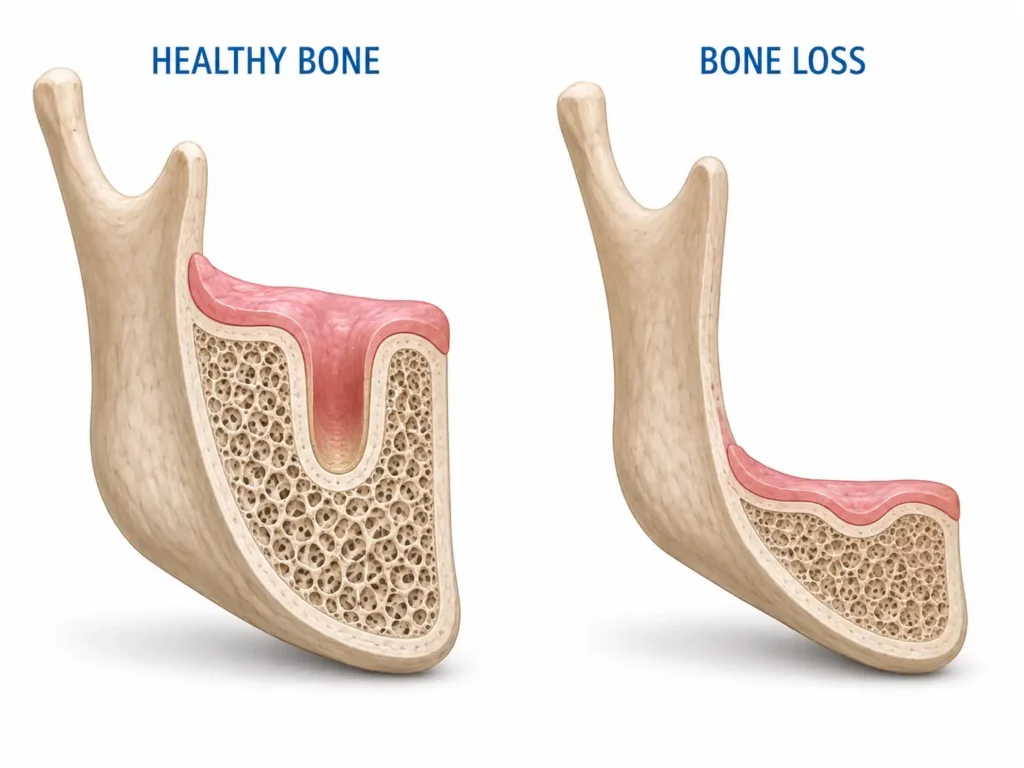

When you lose a tooth, the jawbone in that area starts shrinking almost immediately. The biological reason is simple. The root of a tooth presses against and stimulates the bone every time you chew. That pressure tells your body to keep the bone there. Take the root away and the body interprets the area as no longer needed. It reabsorbs the bone like a slow-motion erosion.
How fast depends on the person. Some patients lose noticeable volume within six months of an extraction. Others hold their bone for years. Smoking, diabetes, gum disease, and certain medications all speed it up. Wearing a denture over the area accelerates it too because the pressure from the denture is distributed across the gum, not focused like a tooth root.
This is why I tell patients that the best time to plan an implant is before you lose the tooth, the second best time is the day the tooth comes out, and the worst time is ten years later when there’s not much bone left to work with.
If you’ve been missing teeth for a while, this is probably what’s going on. It’s not your fault. It’s biology doing what biology does. The good news is that modern implant dentistry has options for almost every scenario.
What “Not Enough Bone” Actually Means
Short answer: It usually means one of three things. Either the bone has shrunk in height (vertical loss), shrunk in width (horizontal loss), or both. The location of the loss matters too because different parts of the jaw need different strategies.
Bone loss is not one thing. When a dentist tells you there’s not enough bone, they could mean any of these:
- The bone is too short vertically. Common in the upper back jaw where the sinus has expanded into the space that used to hold the tooth roots. Also common in the lower jaw where the nerve is now too close to the surface.
- The bone is too narrow horizontally. The ridge has thinned out, making it hard to place a standard implant without the implant being exposed on one side.
- The bone is too soft. Even if the volume looks fine on an X-ray, the actual density may not provide enough grip for an implant to stay stable.
- The bone is gone in a specific zone but fine elsewhere. This is more common than people realize and it changes the whole strategy.
A 3D scan from a CBCT scanner tells us exactly which of these is true for your case. A 2D X-ray cannot. If you were told no based on a 2D X-ray alone, that’s reason enough to get a second opinion.
Your Options When Bone Is the Problem
There are more options than most patients realize. Here are the ones we actually use, ranked roughly by how often they apply to real cases.
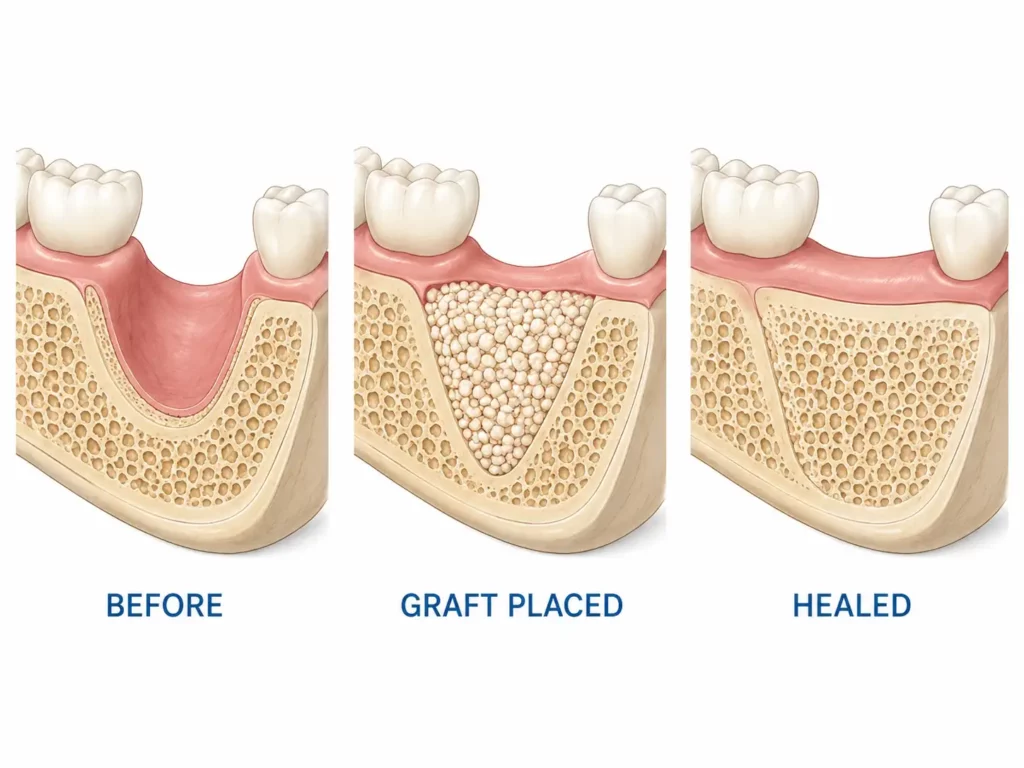
Bone Grafting
The most common solution. Bone graft material is added to the deficient area to rebuild volume. Over the next several months, your body absorbs the graft and replaces it with your own bone. Then the implant goes in.
Graft material can come from several sources:
- Allograft. Donor human bone from a tissue bank. Safe, sterile, well-studied. The most common choice for most cases.
- Xenograft. Animal-derived, usually bovine. Acts as a scaffold for your own bone to grow into.
- Autograft. Your own bone, taken from somewhere else in your jaw. Highest success rate but requires a second surgical site.
- Synthetic alloplast. Lab-made bone substitute. Useful in specific cases.
Most of our grafting cases use allograft or a combination. The choice depends on how much volume needs to be rebuilt and where.
Timeline: Three to six months of healing before the implant goes in. Some cases allow simultaneous graft and implant placement, which shortens this.
Sinus Lift
A specific procedure for the upper back jaw where the sinus cavity has expanded down into where bone used to be. The sinus membrane is gently lifted upward, and bone graft material is placed in the new space below it. After healing, there’s enough bone height for implants.
Sinus lifts are very predictable when done by a trained surgeon. Success rates are very high. This is one of the most common procedures I do for patients told they had no options.
Timeline: Four to nine months of healing, depending on how much vertical bone needs to be gained.
Angled Placement and All-On-X
If you’re missing most or all of your teeth and bone has shrunk across multiple zones, All-On-X dental implants often work without any grafting at all. The implants are placed at angles that use the bone you still have, typically in the front of the jaw where bone tends to last longest.
This is the single biggest reason patients told “no” for traditional implants are still candidates for fixed teeth. The original All-On-4 protocol was designed specifically for this scenario. The modern All-On-X approach refines it further by varying the number of implants based on what each case needs.
If you’ve been wearing a denture, are losing your last few teeth, or had a previous dentist say grafting would be too extensive, All-On-X is worth a serious conversation.
Ridge Expansion
When the bone has enough height but not enough width, the ridge can be split and gently expanded outward to create space for an implant. Sometimes a small amount of graft material is added to fill any gaps. This is less common than grafting or angled placement, but in the right case it’s a great option because the healing is faster.
Mini Dental Implants
Mini implants are narrower than standard implants and can be placed in bone that would not support a traditional one. They’re not right for every case. They work best for stabilizing dentures, replacing small teeth in narrow ridges, or in patients who cannot undergo larger surgical procedures. I’m a member of the International Academy of Mini Dental Implants and use them in cases where they’re genuinely the right answer.
Zygomatic and Pterygoid Implants
For severe upper jaw bone loss where even sinus lifts cannot provide enough foundation, zygomatic implants are anchored into the cheekbone instead of the jaw. Pterygoid implants are placed into a dense bone area at the back of the upper jaw. These are specialized cases. If you’ve been told you need one of these, you’re working with a complex situation that needs careful planning.
I refer cases that need zygomatic or pterygoid implants to colleagues who specialize specifically in those techniques. Knowing when to refer is part of doing this work responsibly.
Which Option Is Right For You?
It depends on five things. None of them can be answered without a 3D scan and a real conversation.
- Where the bone loss is. Upper jaw, lower jaw, front, back. Different zones need different strategies.
- How much bone is left. A little loss is different from severe loss.
- How many teeth you’re replacing. Single tooth, multiple teeth, or a full arch all change the math.
- Your overall health. Smoking, diabetes, certain medications, and bone-affecting drugs can rule certain options in or out.
- What you’re trying to accomplish. Some patients want the most natural-looking result possible. Others want the fastest path to fixed teeth. Both are valid.
The honest answer for most patients is that two or three of the options on this list could work. The job at the consultation is to pick the one that gives the best long-term result for your specific case.
What Might Disqualify You From Grafting Itself
Most patients can have bone grafting. But it’s not for everyone, and a good implant dentist will be upfront about the cases where it isn’t the right call.
You may not be a graft candidate if:
- You take bisphosphonate medications for osteoporosis, especially IV forms, or have taken them in the past. These can interfere with bone healing.
- You have uncontrolled diabetes. The blood sugar swings affect healing dramatically.
- You’re a heavy smoker who cannot or will not cut back for the healing period. Smoking is the single biggest reason grafts and implants fail.
- You have active periodontal disease that hasn’t been treated. We treat that first, then plan grafting.
- You’ve had radiation to the head or neck area in the past. This requires special evaluation.
None of these are automatic disqualifiers. They’re conversation starters. A good consultation goes through your medical history honestly and figures out what’s realistic.
Contact Us to Schedule Free Consultation Today!The Cost of Waiting
This is the part most articles skip and it’s the most important.
Bone loss does not pause while you decide. Every month between losing a tooth and addressing it, the bone in that area continues to shrink. A patient who would have qualified for a straightforward implant in year one may need a sinus lift in year three and a major graft by year seven.
If you’ve already been missing teeth for years, getting started now is still better than waiting longer. The bone loss happening today is changing what’s possible tomorrow. If you’ve been wearing a denture, every year the denture sits on your gums is a year the bone underneath gets thinner.
I’m not trying to scare you into anything. I’m telling you this because patients often delay implant decisions for two or three years thinking they have time, then come back surprised that their options have narrowed. The body is the variable in this equation, not the calendar.
Frequently Asked Questions
The only reliable way is a 3D CBCT scan of your jaw. A standard 2D X-ray cannot accurately measure bone height, width, or density. If you were told no based on a 2D X-ray alone, get a second opinion from a practice that has in-office CBCT. The 3D scan takes a few minutes and gives the actual measurements needed to plan a case.
Not always. Most cases yes, but some patients cannot have grafting because of medical conditions, certain medications, or the location of the bone loss. The good news is that grafting is one of several options, and modern angled placement techniques like All-On-X can often work without grafting at all.
It varies. Small grafts done at the same time as the implant can heal alongside it over three to six months. Larger grafts done before implant placement typically need four to nine months of healing before implants can be placed. Sinus lifts are usually on the longer end of that range.
The procedure is done with local anesthesia and often sedation, so you don’t feel it during. Recovery involves swelling and soreness for the first several days, similar to a tooth extraction. Most patients describe it as much less painful than they expected. We send you home with prescription pain medication and clear instructions for the first week.
In many cases, yes. Modern angled placement, All-On-X, mini implants, and ridge expansion are all techniques that can avoid traditional bone grafting depending on your specific situation. Whether one of these works for you depends entirely on what your 3D scan shows.
The implant will not integrate properly with the bone. It may feel loose, fail entirely within the first one to two years, or cause ongoing bone loss around it. This is why honest planning matters more than rushing into placement. An experienced implant dentist will not place an implant where the bone cannot support it long-term.
Costs vary based on the type and extent of grafting needed, and your specific case. We discuss all costs and financing options during your consultation so you have a clear picture before committing to anything. Most insurance plans cover at least a portion of bone grafting when it’s necessary for implant placement.
Yes, unfortunately. Bone resorption continues as long as there’s no root or implant stimulating the area. The longer you wait, the more bone you lose, and the more complex the eventual solution becomes. This doesn’t mean panic, but it does mean a consultation sooner rather than later gives you more options.
What To Ask Before You Accept “No”
If a dentist has told you implants aren’t possible, ask these specific questions before you settle for something else:
- Was the assessment based on a 2D X-ray or a 3D CBCT scan?
- Which specific bone area is the problem, and how much is missing?
- Did you consider bone grafting?
- Did you consider angled placement or All-On-X?
- Did you consider mini implants?
- If grafting was considered, what would disqualify me from it?
- Are there any specialists you would refer me to for a second opinion?
A dentist who placed implants regularly will be able to answer all of these. A dentist who doesn’t may not be the right person to be making the call about your candidacy.
Why Patients Come to Us for a Second Opinion
Several reasons we hear over and over:
- Their previous dentist did not have in-office 3D imaging
- The case was complex and required techniques beyond their previous dentist’s training
- They wanted to see what All-On-X could do for them specifically
- They were told dentures were their only option and instinct told them to keep looking
- A family member or friend mentioned that we work with cases other dentists pass on
We see implant patients from across Utica, Shelby Township, Sterling Heights, Rochester Hills, and throughout Macomb County. As a Fellow of the International Congress of Oral Implantologists, I plan every case from a 3D scan and give you the honest version, including when something would not be the right call.
Schedule a Real Conversation
If you’ve been told you don’t have enough bone for implants, a second opinion is the right next step. We will take a 3D scan, walk through what your specific bone shows, and tell you honestly whether traditional implants, grafting, All-On-X, mini implants, or something else makes sense for your case. No pressure. No sales pitch. If implants genuinely aren’t right for you, I will tell you that too.
For more on the procedures referenced above, our service pages cover dental implants, All-On-X full arch implants, mini dental implants, and our CBCT 3D imaging capabilities in detail. Related reading: our recent post on how to clean and maintain All-On-X dental implants.
Call us at (586) 731-9240 or reach out through the contact page to schedule your consultation.
Contact Us to Schedule Free Consultation Today!